
Amplifying the Voice of Clinical Neuroscience Medical Student Neurosurgery Training Center |
|

 Does the brain have a true vital sign? Read our latest seminar series post to find out more! Original Lecture by Dr. Uzma Samadani (@DrSamadani) Article by Molly Kearney, Gretchen Koller, Neha Siddiqui, Iyan Younus, Alexander Kelly Introduction Traumatic brain injury (TBI) is the single greatest cause of morbidity and mortality in the United States (US) for people under the age of 35. In the US, 1.4 million people have a TBI each year. Of those patients, 1.1 million are treated and discharged, 235,000 are hospitalized, and 50,000 patients die from their injury.1 Although TBI is becoming more recognized, there are limited diagnostic modalities specific to TBI. TBI outcomes vary significantly based on time until treatment, with delayed treatment and lack of treatment showing very poor outcomes. Since rural populations have fewer healthcare resources and patients must travel greater distances to the nearest hospital, it is not surprising the states with the highest fatality rates are the ones with the most rural populations and little access to Level 1 Trauma centers (i.e. Wyoming, Montana, Louisiana, and Nevada). In contrast, 96% of patients living in Connecticut, Massachusetts, New York, and District of Columbia, areas with better outcomes, live within an hour drive from a Level 1 trauma center. Predictors of TBI Outcomes Multiple factors are important to consider in TBI patients and their prognosis when they present to the Emergency Department (ED), including the following:
Vital Signs Vital signs (VS) reflect essential bodily functions such as blood pressure, heart rate, respiratory rate, body temperature, and blood oxygen saturation. Unfortunately, there is no single vital sign that determines brain function, due to the complex nature of such. Cushing’s Triad is a group of VS that are seen with TBI and include hypertension, bradycardia, and irregular respirations. Hypertension indicates that the body is trying to get blood to the brain; when intracranial pressure is high, the body will increase blood supply to the brain to increase perfusion and oxygenation of the brain. Were the patient to be hypotensive, this would be more indicative of a heart problem rather than a brain injury. Bradycardia and irregular respirations are indicative of brainstem dysfunction. Cerebral Autoregulation Normally, autoregulation of cerebral blood flow is able to maintain a range of systemic blood pressure, or mean arterial pressure (MAP), within the cerebral vasculature between 50-150 mmHg. Unfortunately, in brain injury or stroke, this ability to autoregulate is impaired and the cerebral blood flow becomes proportional to MAP. Glasgow Coma Scale The Glasgow Coma Scale (GCS) is a scoring scale for consciousness which measures functions such as eye opening, motor responses, and verbal responses. It is generally one of the first steps in an examination when a TBI patient arrives at the ED. The problem with this method is that there is a large spectrum of pathology and prognoses at any given GCS score. While this test gives insight into the brain’s function at a specific moment in time, its use as a prognostic tool is low. Physical Examination The physical exam for a TBI includes a thorough neurological assessment, with examination of the pupils, other cranial nerves including gag and corneal reflexes, movement and posture, and looking for any visible injuries of the head. Pupillary deviation can be indicative of the location of injury while corneal reflexes inform the physician about afferent sensation in cranial nerve (CN) V and the efferent function of CN VII. Conjugate gaze deviation, or oculocephalic reflex, also allows for differentiation between lesions of the brainstem and those of the frontal eye fields. Meaning, if the patient’s eyes move within the head during manipulation (i.e. positive oculocephalic reflex), then it is a frontal eye field lesion; if the eyes remain fixed as the head moves (i.e. negative oculocephalic reflex), the lesion is within the brainstem (Figure 1). 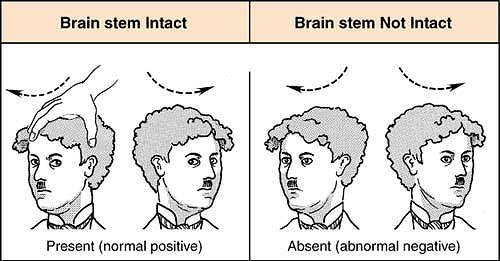 Figure 1: Oculocephalic reflex present when the brainstem is intact (left) vs absent when lesion exists within the brainstem (right). Pupillary Constriction If both CN II and III are intact, both pupils should constrict when a light is shown in one eye. Failure of the pupil to constrict indicates an ipsilateral CN II lesion (loss of direct pupillary light reflex). If the contralateral pupil does not constrict, there is likely a CN III lesion (loss of consensual pupillary light reflex). Posturing There are two types of abnormal posturing that are indicative of a severe brain injury: decorticate and decerebrate posturing (Figure 2). Decorticate posturing occurs due to damage within the internal capsule or higher. A patient who is decorticate may present with flexed arms, clenched fists, extended legs, and internally rotated feet. Decerebrate posturing occurs due to damage at the level of the brainstem and this patient may present with extension of both upper and lower extremities, arched neck, and plantar flexed feet. While posturing does not necessarily describe the brain’s current function, it does allow for classification and/or broad localization of injury. 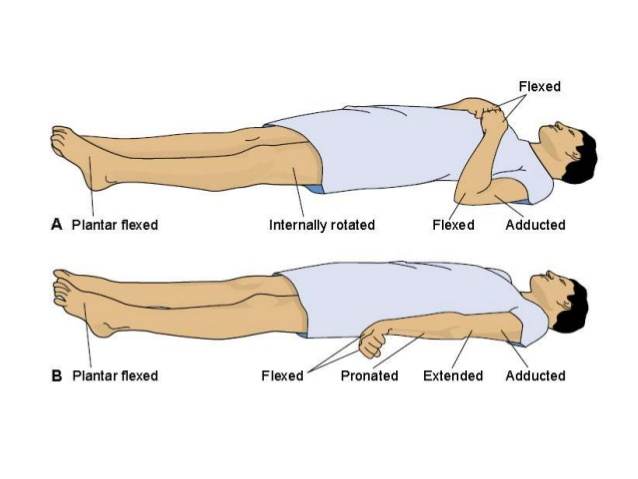 Figure 2: Decorticate (top) vs Decerebrate (bottom) posturing seen in severe brain injuries. Imaging and Analysis After an initial physical exam, the next major step is to obtain imaging, usually in the form of a CT scan, for definitive diagnosis. If the patient is not stable enough to withstand imaging, it is likely they are not stable enough for neurosurgical intervention. An organized, procedural approach to image analysis is effective in diagnosing brain abnormalities. The first step in analyzing a CT scan is assessing the symmetry of the brain. On an axial view, the aqueduct and third ventricle should be midline. Additionally, visualization of the quadrigeminal cistern with intact and visible superior and inferior colliculi indicates that the brainstem is unlikely to be compressed. Finally, a coronal view is used to visualize different types of herniation such as:
Classification of TBI Classification criteria exist for TBI when a patient presents to the ED, but it does not correlate with a better or worse long-term outcome (Table 1). For example, loss of consciousness (LOC) can occur for many reasons, including polytrauma and intoxication; thus, a lack or presence of LOC does not equate with severity of the injury.  Example: A 37 yo woman develops a headache and speech difficulties 2 weeks after a fall. At the ED she is GCS 15 and diagnosed with a subdural hemorrhage. This patient did not meet the requirements for any of the classifications, yet this injury could have been fatal had she not sought treatment.
Diagnosis and Prognosis There is some difficulty in defining exactly what is considered a TBI and what is not as no two brain injuries are the same and similar presentations can have various etiologies. Nonetheless, traumatic brain injuries rated from best to worst prognosis are as follows: scalp injury > skull injury > compressive lesions, epidural/subdural hematoma > subarachnoid hemorrhage/IVH > diffuse axonal injury > anoxic brain injury. Factors correlating with improved outcome after TBI include: younger age/absence of comorbidities, better clinical examinations/GCS, EEG, normoglycemia, motor and sensory evoked potentials, non-rural setting, a dedicated neurological care ICU, higher volume of ICU patients/size of ICU, presence of a full-time neurointensivist, ICP or brain oxygen monitoring, and sedation/paralysis. Intracranial Pressure Bleeding anywhere in the brain has consequences due to blood breakdown products containing neurotoxic substances, such as iron, which can cause inflammation and elevated intracranial pressure (ICP). That being said, a patient’s prognosis does not totally depend on their ICP status, as it is possible to have patients with a very poor prognosis without elevated ICP. Pathologies that may cause an increase in ICP include rapidly expanding lesions (i.e. hematoma, cerebral edema) and hydrocephalus. Other pathologies that may not cause an increase in ICP but may be just as fatal include diffuse axonal injury and anoxic brain injury. Cranial nerves with a longer course are more affected by increased ICP and these changes can be seen on a physical exam. ICP can vary across patients and even within the same patient. A person’s normal ICP is affected by the amount of brain atrophy, number of arachnoid granulations, and amount of loculation, among others. Lazaridis et al. published a paper in 2014 showing that ICP may be different depending on position of the patient, and may even become negative when the patient is standing upright. Finally, ICP may also vary throughout different parts of the brain. With all of this in mind, it can be concluded that ICP is not a standardizable vital sign for the brain. Brain Tissue Oxygenation The purpose of neurocritical care is to maintain oxygen perfusion of the nervous system. Some monitors measure ICP to calculate Cranial Perfusion Pressure (CPP) while other monitors measure brain tissue oxygenation (BtO2; normal > 25, ischemic penumbra between 15-25).The Licox Monitors display local BtO2, but do not describe global brain oxygenation, thus there has not been any Class I evidence showing their use improves outcomes. Although, the BOOST-2 trial did find that treatment based on both ICP and pBtO2 dual monitoring resulted in less hypoxia, as well as a 10% reduction in mortality. Conclusion While the brain may be too complex to be assessed by a single vital sign, a reliable classification system may need to be developed instead. In order to do this, perhaps our approach to understanding the brain should change. New criteria could potentially include imaging, physical exam findings, eye tracking, or even blood-based biomarkers and genetic predispositions. References DHHS, CDC Statistics http://www.cdc.gov/ncipc/tbi/Overview.htm Uncal Herniation. Rebecca Decker https://www.ncbi.nlm.nih.gov/books/NBK537108/#:~:text=Uncal%20herniation%20occurs%20when%20rising,for%20intracranial%20compliance.%5B1%5D Central Herniation. Francis Deng https://radiopaedia.org/articles/central-herniation?lang=us#:~:text=Central%20herniation%20is%20the%20subtype,herniation%20such%20as%20uncal%20herniation. Extracranial Brain Herniation. Francis Deng and Ahmed Abdrabou https://radiopaedia.org/articles/extracranial-brain-herniation?lang=us#:~:text=Extracranial%20or%20transcalvarial%20brain%20herniation,not%20surrounded%20by%20the%20meninges. Tonsillar herniation. Subhan Iqbal and Craig Hacking https://radiopaedia.org/articles/tonsillar-herniation?lang=us#:~:text=Tonsillar%20herniation%20is%20a%20type,herniation%20is%20often%20called%20coning. Crit Care Med. 2001 Mar;29(3):635-40 Neurologic System | Anesthesia Key (aneskey.com) Skill Building: Fearlessly facing neurologic evaluation | Article | NursingCenter Comments are closed.
|
4/6/2021